

Ignoring foot pain rarely makes it go away. Because your feet are the foundation under every step, a sore foot quietly changes how you walk, and that compensation can travel up to your knees, hips, and lower back, shrinking how comfortably you move over months. The real problems with ignoring foot pain are about whole-body mobility, not just your feet, and most are far easier to treat when caught early.
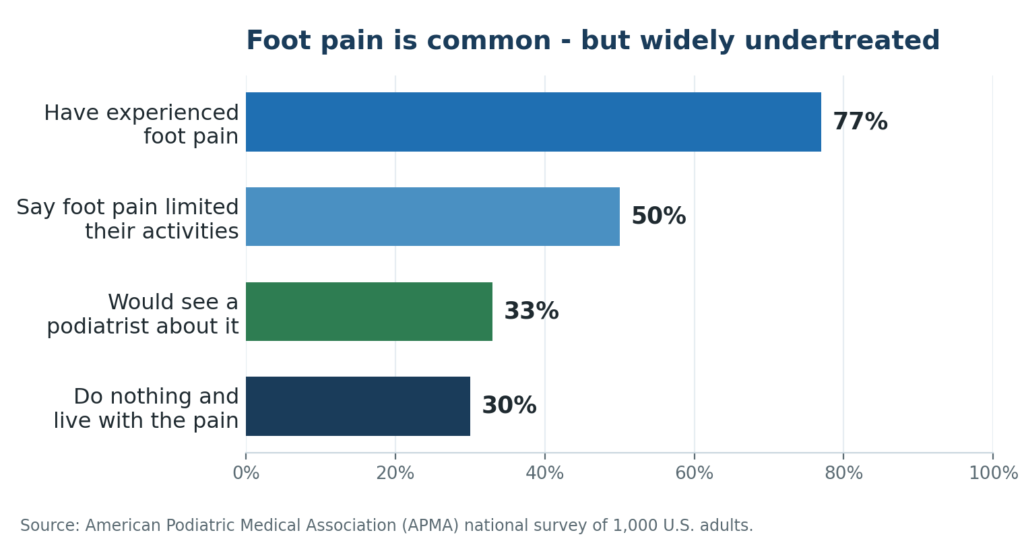
It usually starts small. You swing your legs out of bed, feel a sharp jab in the heel, and tell yourself it is just the shoes. You limp through the first few minutes until it eases, so you wait, a week, then a month. You are not alone in waiting: in a national survey for the American Podiatric Medical Association, 77% of adults said they had experienced foot pain, yet only about a third would see a podiatrist about it, and roughly three in ten do nothing at all. Half said foot pain had limited everyday activities; among those with chronic foot pain, that figure climbs to 83%.
Feet are also good at masking trouble. Many conditions hurt most on the first steps of the day, then ease as the tissue warms up, which makes the problem feel like it is improving when nothing has actually changed. Add the habit of treating sore feet as a normal tax on adulthood or aging, and it is easy to let a fixable problem quietly settle in.
The chain reaction: how foot pain travels upward
Your feet, ankles, knees, hips, and spine work together as one connected system, often called the kinetic chain. Push on one link and the others absorb the difference. When a foot hurts, you instinctively shift weight off the sore spot, shorten your stride, and roll the foot differently. Clinicians call this protective limp an antalgic gait, literally a walk built around avoiding pain.
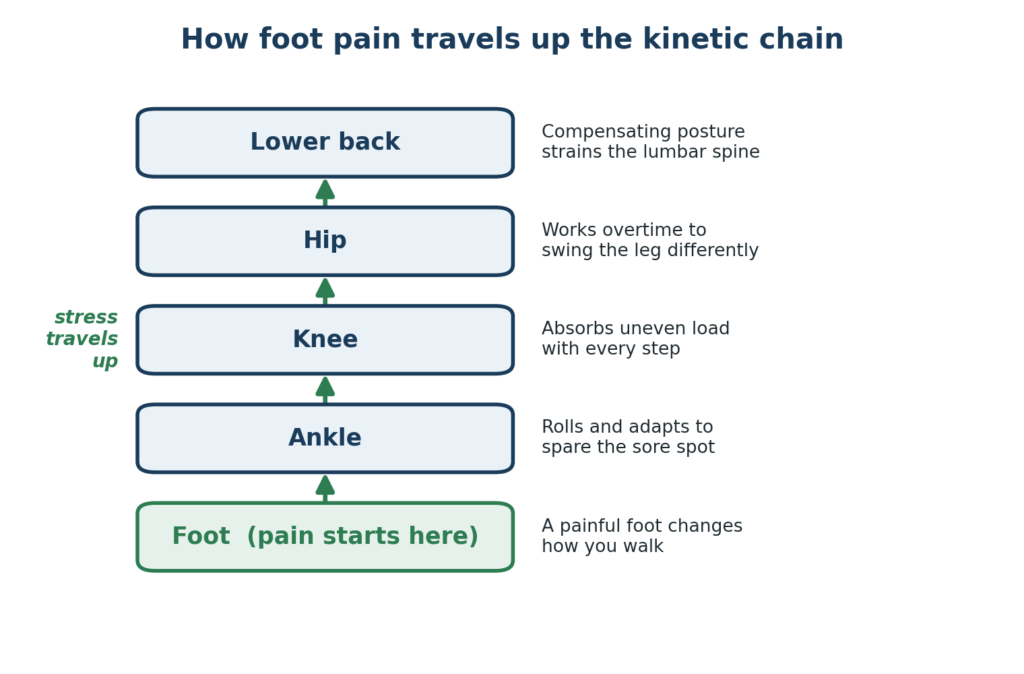
A limp feels small and temporary. Mechanically, it is not. To keep moving while sparing the painful foot, your body asks the ankle, knee, hip, lower back, and opposite leg to do work they were not designed for all day. Mayo Clinic clinicians note that something as ordinary as untreated plantar fasciitis can change the way you walk, which in turn can lead to knee, hip, and back pain, and can make you more sedentary over time. That is why a nagging heel or a stiff big toe often resurfaces weeks later as knee soreness or a cranky lower back: the signal started in the foot, but the bill arrived further up the chain.
What ignoring foot pain can cost you over time
Untreated foot pain rarely stays the same size. It tends to move through stages, and each one is harder to unwind than the last. The pattern below is a general guide, not a diagnosis, but it shows why acting early pays off.
| Roughly when | What is happening | Why it matters |
| First days to weeks | A small limp and guarding; you favor the sore foot without thinking about it. | Tissue is irritated but usually still flexible. The easiest, cheapest point to fix. |
| Weeks to months | The altered gait becomes a habit. Secondary aches appear in the ankle, knee, hip, or back, and the original problem can turn chronic. | Many foot conditions are far easier to treat early. Once a pattern sets in, recovery typically takes longer. |
| Months to years | You move less to avoid discomfort. Strength, balance, and conditioning slip, and overloaded joints may develop wear and inflammation. | Reduced activity affects weight, heart health, and independence, and in older adults it raises the risk of falls. |
Foot pain, mobility, and falls in older adults
The stakes rise with age. In the long-running Framingham Foot Study, about 19% of older men and 25% of older women reported foot pain on most days, and broader estimates place foot pain in older adults somewhere between 18% and 42%.
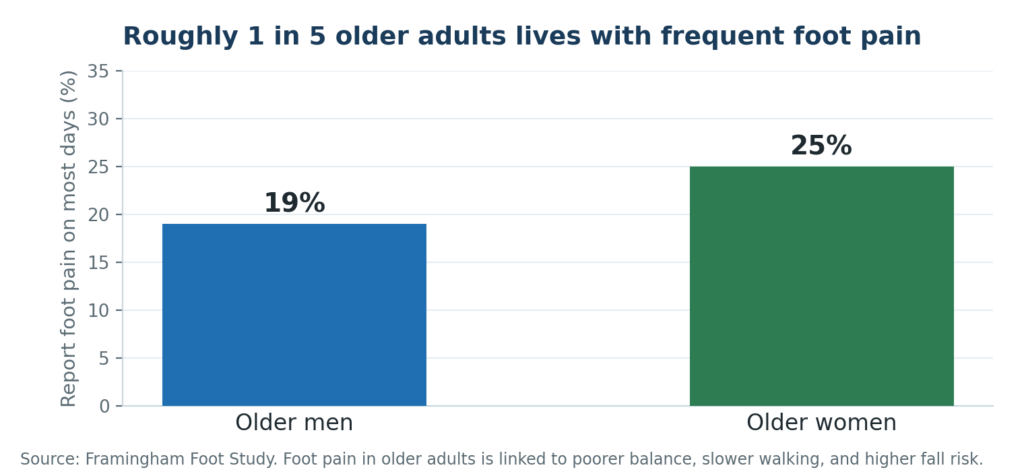
That matters because foot pain in older adults is tied to measurable problems with walking, balance, and rising from a chair, and to a higher risk of falls. Sore feet that quietly keep someone sitting down do not just hurt; they chip away at the strength, balance, and confidence that protect independence. Treating foot pain early is part of protecting mobility for the long run.
When to see a podiatrist
Some foot pain settles with a few days of rest and better shoes. Other signs are your body asking for help now. Do not wait out any of the following:
- Foot pain that lasts more than a week or two, keeps returning, or is getting worse
- Pain severe enough that you cannot put weight on the foot or walk normally
- Swelling, warmth, or redness, or pain that follows a fall, twist, or injury
- Numbness, tingling, or a burning feeling, especially if it is spreading
- Any sore, blister, or color change that is slow to heal, particularly if you have diabetes
Diabetes deserves special caution. The CDC notes that nerve damage can dull the pain that would normally warn you of an injury, so a small wound can go unnoticed, become infected, and in serious cases lead to amputation. For people with diabetes, daily foot checks and prompt care are not overkill; they are how limbs are saved.
Conditions that quietly escalate
Part of why ignoring foot pain backfires is that the everyday conditions behind it tend to progress when left alone:
- Plantar fasciitis (heel pain). Often responds well to early, conservative care, but left unchecked it can linger for many months and drive that pain-avoiding limp.
- Bunions and hammertoes. Structural changes that are progressive by nature. As the joint drifts, shoes get harder to wear and your weight shifts, feeding back into how you walk.
- Neuromas and metatarsalgia. Nerve and pressure pain in the ball of the foot that can intensify and start dictating which shoes and activities feel tolerable.
- Achilles tendonitis and ankle issues. Tendon and joint problems that tend to stiffen and weaken the more they are worked around rather than treated.
- Diabetic neuropathy. Here the absence of pain is the danger; numbness means injuries can be missed entirely, which is why it needs regular professional monitoring.
The good news: early care changes the trajectory
Because foot pain follows a fairly predictable path, catching it early usually means simpler, less invasive treatment and a faster return to normal movement. Most foot pain is first addressed with conservative, well-established measures:
- Relative rest and activity changes to calm the irritated tissue
- Supportive, properly fitted footwear and, when helpful, custom orthotics to correct the mechanics driving the pain
- Targeted stretching, strengthening, and physical therapy to rebuild a balanced gait
- Icing and short courses of anti-inflammatory measures where appropriate
When pain is stubborn or a structural problem is involved, a podiatrist can discuss more advanced options. These may include regenerative approaches such as class IV laser therapy and shockwave therapy, or minimally invasive, in-office procedures for issues like bunions and hammertoes. Evidence for regenerative therapies is still developing, results vary, candidacy depends on your diagnosis, and insurance coverage differs, so these are evaluated case by case rather than treated as guaranteed fixes. The point is simply that you have far more, and gentler, options when you act early than when you wait for a foot problem to reshape your whole stride.
Simple steps you can take this week
These can ease mild, recent foot pain and are reasonable while you arrange an evaluation. They are general self-care, not a substitute for a professional exam, and they do not replace urgent care if you have any of the warning signs above.
- Switch to supportive shoes. Retire the flat, worn-out, or unsupportive pairs for now; cushioning and arch support reduce strain while tissue settles.
- Respect the pain, do not push through it. Sharp or worsening pain is a stop sign. Ease off the activity that triggers it rather than gritting your way forward.
- Stretch the calf and the bottom of the foot. Gentle, regular calf and plantar fascia stretches can relieve the tension that pulls on the heel, especially first thing in the morning.
- Ice after activity. Ten to fifteen minutes of icing after time on your feet can calm inflammation. Use a barrier so ice never sits directly on skin.
- Check your feet daily if you are diabetic. Look at the tops, bottoms, and between the toes for cuts, blisters, redness, or color changes, and report anything that is not healing.
Frequently asked questions
How long should I wait before seeing a podiatrist for foot pain?
A good rule of thumb is more than a week or two of pain, pain that keeps returning, or pain that interferes with normal activity. See someone sooner if you have diabetes, numbness, swelling, a wound, or cannot bear weight.
Can foot pain really cause knee, hip, or back pain?
Yes. When a sore foot changes how you walk, the added stress travels up the kinetic chain to the ankle, knee, hip, and lower back, which is why those areas can start to ache even though the foot is the source.
Will ignoring foot pain make it harder to treat later?
Often, yes. Many foot conditions respond best to early, conservative care. Once an altered gait becomes a habit and the problem turns chronic, recovery usually takes longer and may need more involved treatment.
Is foot pain just a normal part of getting older?
Foot pain becomes more common with age, but common is not the same as normal or unavoidable. It is treatable, and addressing it matters because foot pain in older adults is linked to balance problems and a higher risk of falls.
My foot feels numb but doesn’t hurt, and I have diabetes. Should I worry?
Numbness is a warning sign, not a reassurance. It means an injury could go unnoticed and become infected. Check your feet daily and have new numbness or any non-healing sore evaluated promptly.
What happens at a first visit for foot pain?
Expect a history, a hands-on exam, and a look at how you walk, plus imaging if needed. From there you receive a personalized plan, which usually starts with the least invasive options that fit your diagnosis.
Book a consultation
If foot pain is changing how you walk or keeping you from the things you enjoy, an early evaluation can save you months of compensating later. Request an appointment with a podiatrist in Hoffman Estates at the Comprehensive Foot and Ankle Institute, or call (847) 310-1600.
Medical disclaimer: This article is for general educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified provider about your condition. Results vary by patient and cannot be guaranteed.
Medically reviewed by Dr. Sutpal Singh, DPM, FACFAS — double board-certified foot and ankle surgeon (FACFAS) with 30+ years of experience, Comprehensive Foot and Ankle Institute, Hoffman Estates, IL.
References
- American Podiatric Medical Association (APMA) — national survey on foot pain prevalence and care-seeking.
- Mayo Clinic Health System — Heel pain might be plantar fasciitis.
- Menz HB, et al. — Foot Pain and Mobility Limitations in Older Adults: The Framingham Foot Study.
- Awale A, et al. — Foot Function, Foot Pain, and Falls in Older Adults: The Framingham Foot Study.
- Centers for Disease Control and Prevention (CDC) — Diabetes and Your Feet.

